On January 6th 2022, the Department of Health and Human Services (HHS) made significant changes to the guidelines by which hospitals report COVID-related statistics. New fields were added, and several fields were dropped. HHS mandates that these new changes be complied with by February 2nd. But these changes don’t seem benign to me — they risk misinterpretation and overstatement of the level of worry we should have about serious COVID in America’s youngest. And two full years into the pandemic, HHS missed yet another easy, obvious opportunity to help us better distinguish between worrisome and non-worrisome cases.
HHS has required that hospitals report key indicator data for a long time. They make adjustments to what is required from time to time. That is not new. But what is new is that they are now requiring several additional fields related to pediatric patient statistics that in aggregate risk the creation of alarming new headlines in a month or two, specifically about pediatric COVID. At the same time, HHS is also dropping the requirement that America’s hospitals report daily COVID-19 deaths. Yes, you read that right; it’s a very surprising directive; we’ll get to that in a moment.
The net result of these changes: we will likely soon see media reports along the lines of “Pediatric COVID Hospitalizations Rise Alarmingly,” and “Pediatric ICU Beds Near Capacity,” when the underlying truth is that worrisome COVID among our youngest adults has been, and remains, extremely low — at the level we should worry about seasonal influenza.
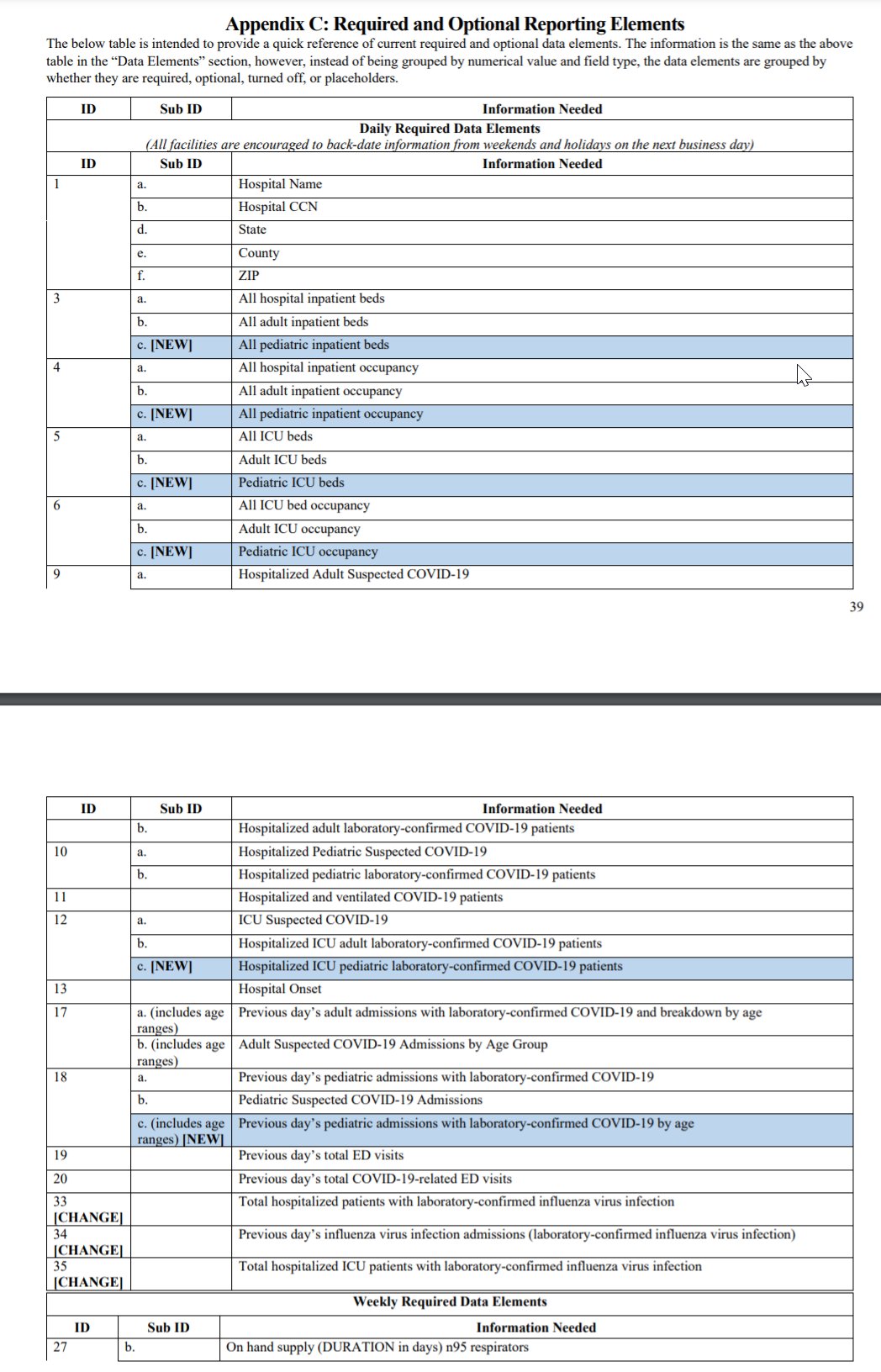
What new data does HHS now want? They’re highlighted in blue in the screenshot below [source: COVID-19 Guidance for Hospital Reporting and FAQs (hhs.gov).]
Needless to say, the downstream impact of overstating the severity of pediatric cases can be very significant. It “bolsters” the case for unnecessarily prolonged mandates, school and college restrictions, elimination of activities, mandated boosters, masking, and yanking yet more childhood away from those who have always been least at risk of severe outcomes. Kids have inarguably already paid an enormous price in their childhood and mental health toward COVID mitigation, and it’s important that we get the most accurate picture of risks to them to chart the path of least overall harm. This reporting change and the downstream misinterpretations are quite likely to prolong it.
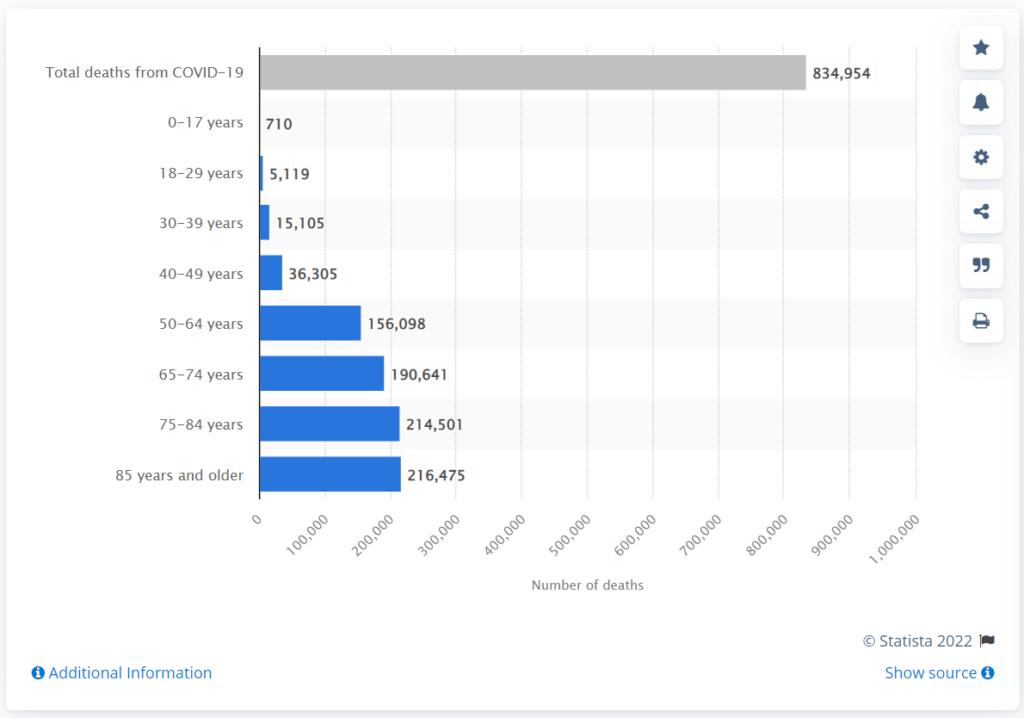
The risk to 0-18 year-olds of severe outcome due to COVID is exceedingly low. At this writing, of the more than 850,000 Americans who have died with or from COVID, the number of 0-18 year-olds who have died with or from COVID stands at fewer than 900. Kids are at greater risk of dying from suicide and vehicular accidents than COVID. They’re not at zero risk, but their infection fatality rate due to COVID is below 0.003%. Every day, when we drive our kids on the highway, we’ve decided that the risk/reward tradeoff is worth it, and that while highway danger is present, it’s not so alarming as to keep everyone home forever.
Overall, risk of fatality due to COVID is lowest for our youngest. Luckily, we as a society now generally understand that. But we still greatly underestimate just how age-weighted COVID is.
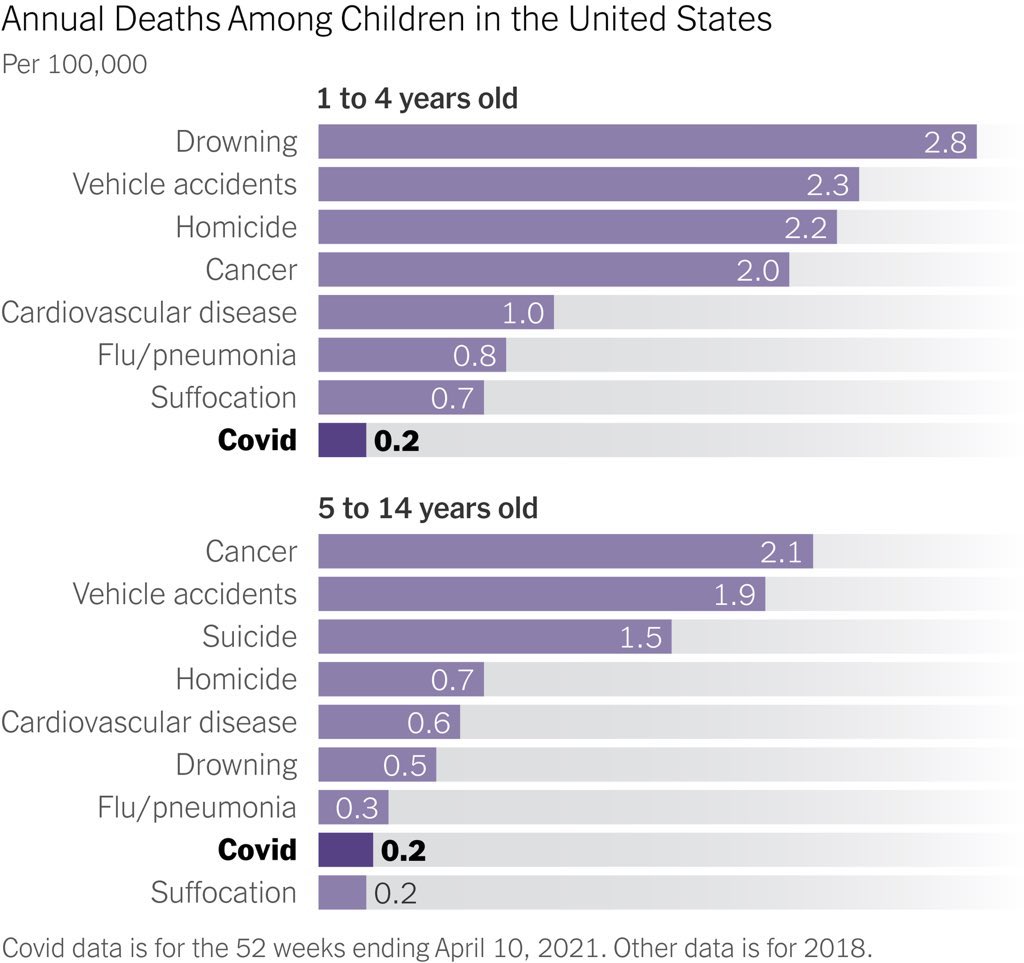
The New York Times visualized CDC mortality risk data this way, back in May of 2021:
But now, because hospitals are being required to report pediatric ICU beds and the number of pediatric patients in ICU with COVID, it will tend to make for easy, alarming click-bait headlines.
How so? Well, let’s say you’re operating a medium-sized hospital. More than a year ago, your hospital wisely instituted a policy during this infectious pandemic: all admitted patients are to be tested for COVID, regardless of whether they show symptoms.
That’s precisely as my own local hospital has instituted (see purple highlighted text); I encourage you to take a moment to check your own:

That’s a wise policy; I have no problem with that.
But here’s how that, plus the new metrics above, add fog. Let’s say you have 5 ICU beds dedicated to your pediatric wing. A recent icy weekend has caused four of those beds to be occupied: two by kids with broken bones for serious injury, one for a grave car accident, and one who has presented for appendicitis. Note that zero of them presented to the hospital because of COVID, but upon mandatory routine testing, it was detected that four of them are asymptomatically COVID-positive because there’s an outbreak in your region at the moment.
Your accurate reporting to HHS, under these new guidelines, will be that 80% of your pediatric ICU beds were taken up by COVID patients. Now, sum that same scenario up from thousands of hospitals across the country, and render it on a nice-looking dashboard. Journalists from around the country will read the dashboard and rush to their media feeds with semi-accurate but extremely misleading headlines: “80% of Pediatric Beds Taken Up By COVID Patients,” or “Alarming Rise in Serious COVID Cases in Young Adults.” Animated infographics will show that pediatric COVID is on a sharp rise because, at a minimum, hospitals weren’t required to break out this data before. Scary infographics will course through social media, and be trotted out by the largest teachers unions and other “let’s close the schools” advocates.
Most maddeningly, HHS is entirely passing up an easy opportunity to actually differentiate between worrisome cases and non-worrisome cases. It’s as simple as this: Did the patient present to the hospital because of COVID-like symptoms, or not? Doctor, nurse or even patient — check a box. Then, allow the slicing and dicing based upon that key variable. Yet here we are, two years into this pandemic, and HHS is not even attempting to ask hospitals to start reporting whether patients are in the hospital because of COVID, or whether they incidentally tested positive.
It’s not like this is some kind of secret revelation, unknown to officials. People like me have been pointing the “with vs. from” distinction out for more than a year. And finally, even Dr. Fauci admitted in late December 2021 that these two conditions, incidental vs. causal, are quite different, explaining it as though it were a new concept:
It’s not just what HHS is adding, it’s what reporting requirements they are dropping. I want to draw your attention to these five in particular:
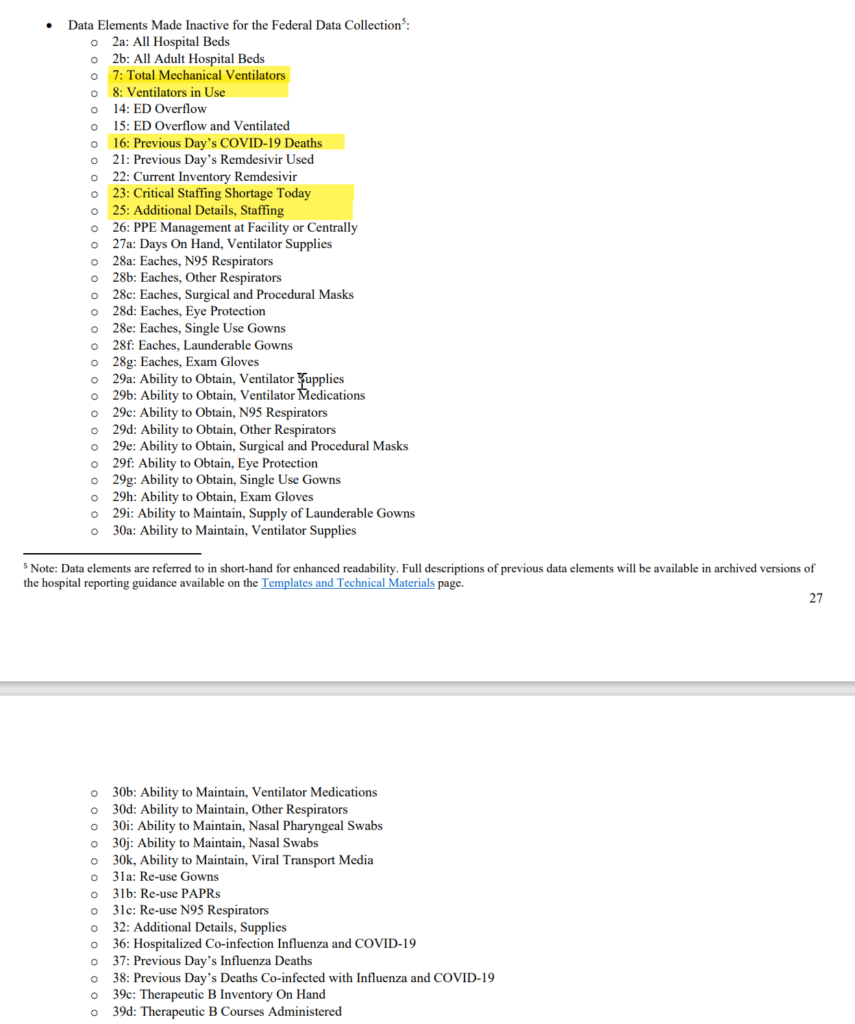
HHS is removing the requirement that hospitals report the prior day’s death with COVID-19. Daily deaths will still flow through to the CDC via a separate process, but removing daily death counts will make it much harder to separate worrisome cases from non-worrisome cases, because we won’t be able to see infection-fatality-rates for same-hospital data. We also won’t be able to know that zero patients are on ventilators, for instance — another (old) indication of severity.
Note too that HHS is shielding from reporting the need for hospitals to disclose anything about staffing shortages — both the quantity and explanatory fields. It cannot go unnoticed that a substantial cause of many staffing shortages (NPR) at hospitals and elsewhere has been the imposed mandates that they be vaccinated. More here (Business Insider, and here (WSJ).
So, why these changes? As always, I must ask — who benefits by obscuring this picture? I have some hypotheses. But I’ll leave that exercise for now, to the reader.